(425) 228-3187
(425) 228-3187
DIEP FLAP FAQ’s
Implant Reconstruction FAQ’s
Most women are candidates for 2-stage tissue expander to implant reconstruction, and, less often, direct to implant reconstruction. Implants are the most common form of breast reconstruction in the world. Those patients typically favoring implants over the DIEP or PAP flap include those with very little abdominal tissue, those who would like to minimize the amount of scars they have (especially on their abdomen), or those women who have not completed child-bearing. Though they are performed by a greater number of plastic surgeons compared to the DIEP flap, they are not necessarily the best option for every patient.
Many patients may be candidates for consideration of direct-to-implant reconstruction. This is a very appealing option to patients, but we have learned that this rarely results in the “one and done” operation patients are desiring. Most patients who undergo direct-to-implant reconstruction will undergo at least one revision operation in the future.
This ultimately depends on your goals. Women who undergo radiation (before or after implant placement) face higher complication rates (including loss of reconstruction) and are less happy with their result, especially when compared to those who received a DIEP flap. This has to do with many issues, but, simply, the breast is much harder to reconstruct with implants when it has been irradiated. There is also significantly more risk when attempting to do so. Many times, supplementation with non-radiated tissue (either a latissimus dorsi flap from your back, or considering complete reconstruction with the DIEP flap with or without implants) leads to an improved and more natural appearance of the reconstructed breast.
While implants are some of the most scrutinized medical devices on the market, they are safe and widely used in breast reconstruction and augmentation. As long as you understand the risks of implants and are a candidate for their use, they can be utilized for your breast reconstruction. The best way to determine whether implants are appropriate for you is through a thorough discussion of your goals and desires with Drs. Bailey, Hutter or Morton.
Of note, The FDA has placed a “black box warning” on breast implants (updated September 2020), requiring that patients be informed of their potential risks prior to implantation. These warnings include:
- Breast implants are not considered lifetime devices;
- The chances of complications increases over time;
- Some complications require more surgery;
- Breast implants have been associated with the development of a cancer of the immune system called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL);
- BIA-ALCL occurs more commonly in patients with textured breast implants than smooth implants, and deaths have occurred from BIA-ALCL;
- Breast implants have been associated with systemic symptoms.
Drs. Hutter, Bailey and Morton generally do not recommend the use of textured devices because of the reported risk of BIA-ALCL. This includes your tissue expander, should you require one. Please discuss this further with them at your consultation.
Some postoperative complications including infections can be more serious when you have an implant in place. When there is concern that your implant is infected, Drs. Bailey, Morton and Hutter typically recommend returning urgently to the operating room to wash out the implant pocket with antibiotics. You will also likely be admitted to the hospital for intravenous antibiotics. While implant infections are difficult to treat with the prosthesis in place, every effort is made to save your implant. Of note, an infection following a DIEP flap is typically not as serious as with an implant, as there is no foreign body in place.
Silicone and saline implants are both available for use in breast reconstruction. Both are constructed with a silicone shell, so there is no truly “silicone free” implant. In general, Drs. Hutter, Bailey and Morton recommend smooth (not textured) silicone implants for breast reconstruction. Silicone implants are more natural in feel and appearance and have less risk of rippling (causing visible ripples in your breast).
Drs. Morton, Bailey and Hutter typically take a “prepectoral approach”, which is defined as placing tissue expanders and implants above the muscle. This minimizes postoperative pain, reduces the mobility of your implant after surgery and ultimately results in a more natural appearance.
Many times we use cadaver skin/acellular dermal matrix to improve the shape and overall aesthetics of your reconstructed breast. Drs. Hutter, Morton and Bailey make a decision in the operating room as to whether or not you would benefit from this product. They use acellular dermal matrix more often when you may receive radiation after surgery, or when you are undergoing direct to implant reconstruction. When a tissue expander is placed in preparation for a DIEP flap, acellular dermal matrix is almost never used as it offers little benefit in this scenario.
Capsular contracture occurs when your body, over a period of years, forms a tight scar around your breast implant. This results in a very unnatural appearing “stuck on” reconstructed breast. This is a very difficult problem to fix, and almost always requires an additional operation (which is why we want you to know implants are not lifetime devices and may require further surgery years after completing your reconstruction). When capsular contracture recurs after surgical repair, we generally recommend having the implant removed and “going flat” for a period of 6-12 months prior to considering further reconstruction. The only way to avoid the risk of capsular contracture is to not have implants.
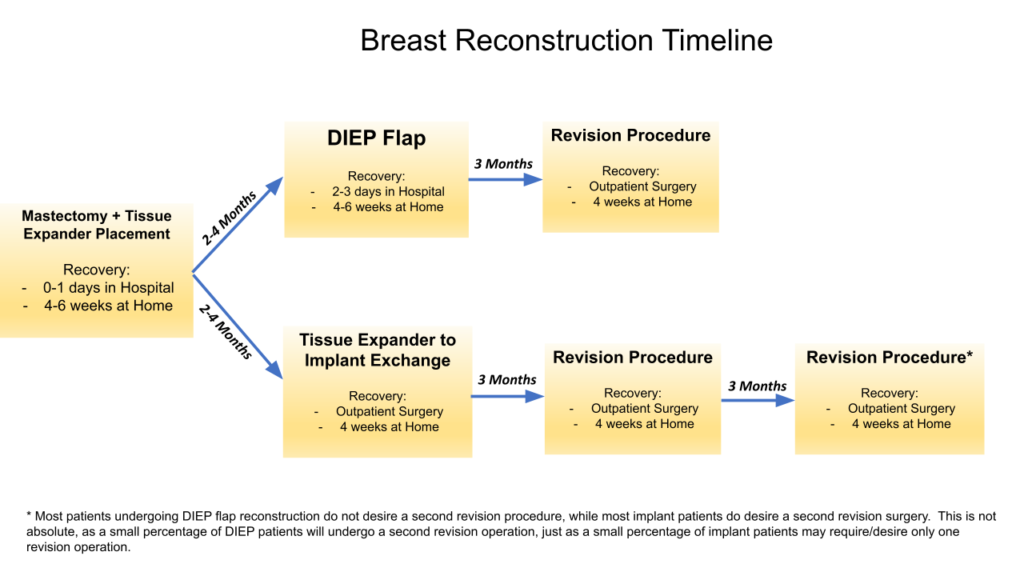
This is a common misconception. The amount of time consumed by implant based reconstruction is typically longer than that of DIEP flap reconstruction. Breast reconstruction is a 1 year process from time of diagnosis to completion of reconstruction, and more time is required to perform implant reconstruction due to the increased number of revision procedures required to “fine tune” or “touch up” implants and the recovery period involved with each of these operations. Please see the table below outlining the typical recovery timeline for each method of breast reconstruction for more information.
Reconstruction Revision
Lumpectomy Repair
Hybrid/Combined Reconstruction
PAP Flap
Have Any Other Questions?
Talk to the professionals at Plastic & Reconstructive Surgeons about how we can help meet your wants or needs. Contact us or call today to schedule your consultation at (425) 228-3187.